Migraine, Headache and Medical Marijuana (Cannabis)

Charles Booras, MD
SHARE
Migraine, Headache and Cannabis
Summary:
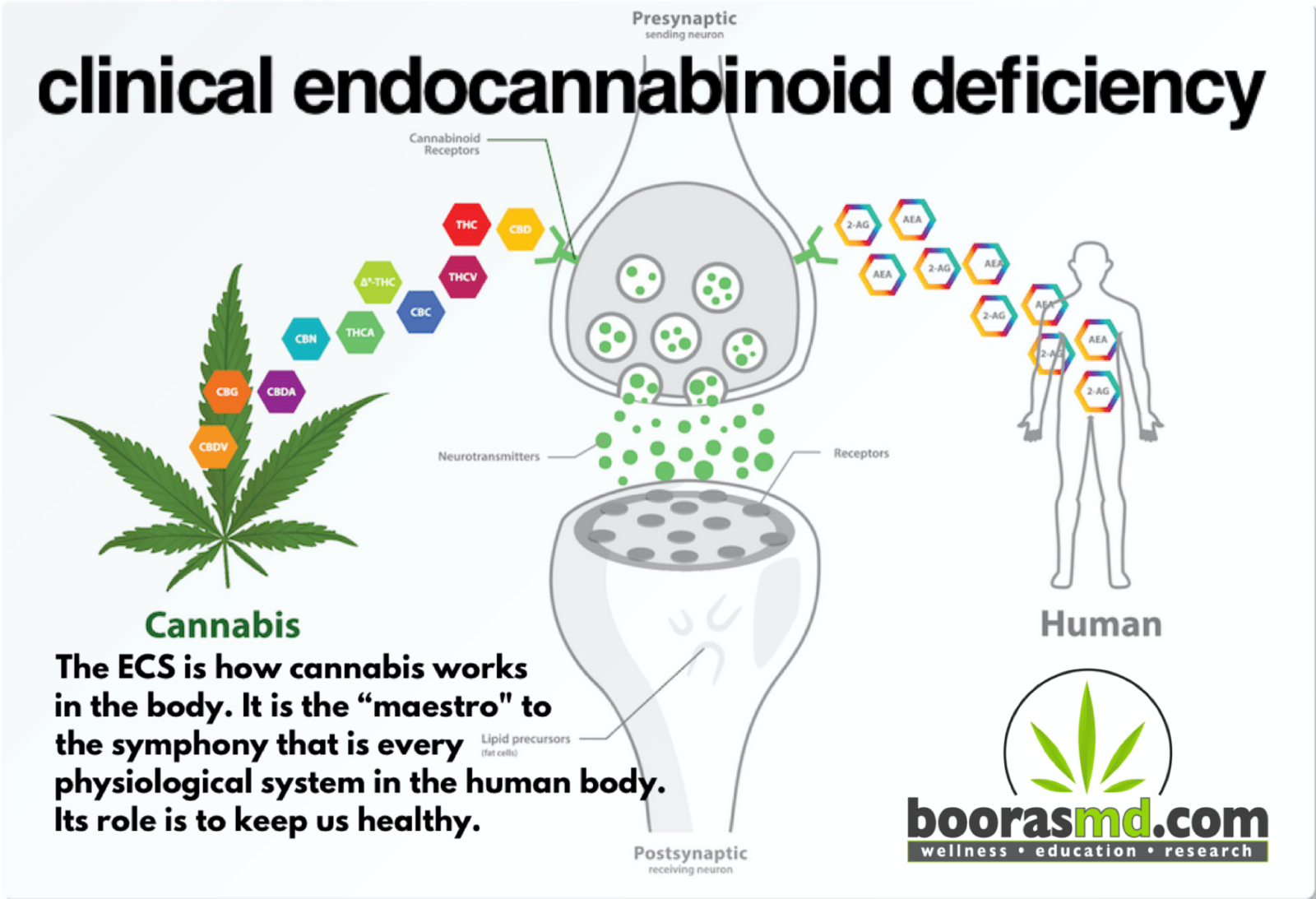
- Emerging evidence suggests that migraine is yet another disorder resulting from a Clinical Endocannabinoid Deficiency (CECD). Anandamide is one of two known endocannabinoids made by humans to activate the Endocannabinoid System (ECS). Anandamide functions in the brain in a fashion similar to how anti-migraine medications work. https://boorasmd.com/education/articles/clinical-endocannabinoid-deficiency/
- Migraine (along with other conditions like fibromyalgia and irritable bowel syndrome ) display common clinical, biochemical and pathophysiologic patterns that suggest an underlying Clinical Endocannabinoid Deficiency. These conditions are challenging to treat, but do respond favorably to medical cannabis.
https://pubmed.ncbi.nlm.nih.gov/15159679/
Conventional treatment:
1. Abortive therapy.
-
- Triptans (Imitrex, Relpax, Maxalt, etc).
- Ditans (Reyvow). A new class of agents different than Triptans as they will not cause vascular narrowing.
- Gepants (Aimovig, Emgality, Ajovy, Vyepti, etc). These are calcitonin gene-related peptide (CGRP) receptor antagonists, administered subcutaneously once a month (Vyepti is every 3 months). These have preventive benefits also.
- Pain medication (opioids, barbiturates).
- Ergot alkaloids (Migranal, DHE-45, Ergomar, etc).
- Nonsteroidal anti-inflammatory Drugs (NSAID’s, such as Ketorolac, Celebrex, Naproxen, Ibuprofen, etc).
- Anti-nausea medication (Zofran, Phenergan).
2. Prophylactic (Preventive) therapy.
-
- Anti-convulsants (Topamax, Depakote).
- Beta blockers (Propranolol, Timolol).
- Tricyclic antidepressants (Elavil, Doxepin, Nortriptyline, Protriptyline, etc).
- Calcium channel blocker’s (Verapamil, etc).
- Selective serotonin reuptake inhibitors (SSRI’s). This family includes Prozac, Paxil and Sertraline. Effexor is an SNRI, which also helps prevent migraine.
- CGRP inhibitors (see Gepants above).
- BoTox injections.
Medical Cannabis:
- The first reported use of cannabis was in a Chinese pharmacopeia from 2600 BC! I’m sure some of these early users suffered with headache.
- Cannabis works via activation of the mammalian Endocannabinoid System (ECS). This system inhibits the release of neurotransmitters involved in the transmission of pain signals. It appears that medical cannabis reduces both the physiologic and inflammatory components of pain that appears to be involved in migraine attacks.
https://pubmed.ncbi.nlm.nih.gov/20353780/
- In a study of 2032 patients, headache was a symptom treated with cannabis in 25%. Almost 90% of the headache cohort were treating migraine. There was a significant reduction and use of prescription pain medication, including opioids, antidepressant, anti-anxiety, triptans, NSAID’s, anticonvulsants, muscle relaxants and Ergots.
https://pubmed.ncbi.nlm.nih.gov/29797104/
- Use of cannabis to alleviate headache and migraine is relatively common, yet research on its effectiveness remains sparse. We sought to determine whether inhalation of cannabis decreases headache and migraine ratings as well as whether gender, type of cannabis (concentrate vs flower), delta-9-tetrahydrocannabinol, cannabidiol, or dose contribute to changes in these ratings. Finally, we explored evidence for tolerance to these effects. Archival data were obtained from Strainprint, a medical cannabis app that allows patients to track symptoms before and after using different strains and doses of cannabis. Latent change score models and multilevel models were used to analyze data from 12,293 sessions where cannabis was used to treat headache and 7,441 sessions where cannabis was used to treat migraine. There were significant reductions in headache and migraine ratings after cannabis use. Men reported larger reductions in headache than women and use of concentrates was associated with larger reductions in headache than flower. Further, there was evidence of tolerance to these effects. https://www.jpain.org/action/showPdf?pii=S1526-5900%2819%2930848-X
- “There is accumulating evidence for various therapeutic benefits of cannabis/cannabinoids, especially in the treatment of pain, which may also apply to the treatment of migraine and headache. There is also supporting evidence that cannabis may assist in opioid detoxification and weaning, thus making it a potential weapon in battling the opioid epidemic. Cannabis science is a rapidly evolving medical sector and industry with increasingly regulated production standards. Further research is anticipated to optimize breeding of strain-specific synergistic ratios of cannabinoids, terpenes, and other phytochemicals for predictable user effects, characteristics, and improved symptom and disease-targeted therapies.”
https://pubmed.ncbi.nlm.nih.gov/30152161/
Additional References:
- https://pubmed.ncbi.nlm.nih.gov/29615860/
- https://pubmed.ncbi.nlm.nih.gov/30405366/
- https://pubmed.ncbi.nlm.nih.gov/29770251/
Written by Charlie Booras, MD on 9/9/20.